Case history- 4
5 October, 2021
" This is an online E- log book to discuss our patient's de- identified health data shared informed after taking his/ her guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E- log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome."
A 65 year old male patient came to OPD with chief complaints of swelling of the legs and facial puffiness since 5 days.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 5 days back and then he noticed swelling of lower limb which is progressed to upper limb and also facial puffiness.
No history of fever, vomitings, loose stools, decreased urine output and orthopnea.
PAST HISTORY:
Patient is a known case of CVA (Cerebrovascular accident) 2 months back and recovered within 1 week.
Slurring of speech is seen.
He is a hypertensive patient since 5 months.
He had undergone 2 sessions of hemodialysis 8 years back.
No history of diabetes, CAD, asthma, TB, epilepsy, thyroid disorders.
No history of surgeries in the past.
PERSONAL HISTORY:
Appetite: normal
Diet: mixed
Sleep: adequate
Bowel and bladder movements: regular
Micturition: normal
Addictions: 90 ml alcohol for 3 days and
17 beedi/ day
FAMILY HISTORY:
No member in the family have similar complaints.
TREATMENT HISTORY:
Patient had not undergone any treatment prior.
He is not allergic to any known drugs.
GENERAL EXAMINATION:
Patient is conscious, coherent, cooperative and well oriented to time, place and person.
There is no signs of pallor, icterus, cyanosis, clubbing and generalised lymphadenopathy.
There is bipedal edema of pitting type.

VITALS:
Temperature: 98.4° F
Blood pressure: 220/ 130 mm of Hg
Respiratory rate: 24/ min
Pulse rate: 70/ min
SPO2: 98% at room temperature
GRBS: 127 mg%
SYSTEMIC EXAMINATION
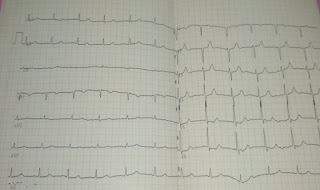
CARDIOVASCULAR SYSTEM:
No thrills
S1 and S2 sounds are heard
No cardiac murmurs
RESPIRATORY SYSTEM:
No dyspnoea
No wheezing sounds
Position of trachea - central
Breath sounds- vesicular
ABDOMEN:
Shape of abdomen- scaphoid
Tenderness- no
Palpable mass - no
Hernial orifices- normal
Free fluid- no
Bruits- no
Liver - not palpable
Spleen- not palpable
Bowel sounds- yes
CENTRAL NERVOUS SYSTEM:
Level of consciousness: conscious
Speech: normal
Signs of meningeal irritation
Neck stiffness- no
Cranial nerves - normal
Motor system- normal
Sensory system- normal
INVESTIGATIONS:
BLOOD UREA




Comments
Post a Comment